There are lots of things happening around the coronavirus epidemic – sorry, it’s a pandemic now – but most of them revolve around issues we’ve already addressed in earlier articles here, and others have addressed ad nauseam elsewhere. Still, it’s good to have accurate, insightful information on which to base our own decisions and actions, and that’s what I try to present here.
Let’s start with the situation in health care. It’s looking pretty dire. Italy has so many cases of the disease that doctors have advised medics to “stop treating the elderly and focus on those with better survival chances“. That’s really hard to hear if you, like me, are officially classified – even if just barely – among the “elderly” to whom they’re referring.
Guidance published by a top Italian health agency has now suggested that rather than admit patients on a “first come first served” basis, hospitals should swap to “catastrophe medicine” guidelines.
These guidelines are typically used in war zones and during natural disasters.
If a limit on beds is implemented it could mean elderly patients with no signs of coronavirus being turfed off ICU wards to make space for younger patients who have longer left to live.
There’s more at the link.
Folks, if you’re thinking “Well, that’s Italy. It’ll never happen here!”, then you need to reassess your thinking right now, if not sooner. When the numbers get high enough, this sort of triage will, repeat, WILL happen here. The sheer volume of patients will make it inevitable, particularly when aggravated by a desperate shortage of health care personnel (see next citation). When supplies and care are both short, those best able to benefit from them, and whose recoveries will best benefit society, will get priority. The rest of us will be S.O.L.
Oh – and about shortages of health care personnel:
As the U.S. battles to limit the spread of the highly contagious new coronavirus, the number of health care workers ordered to self-quarantine because of potential exposure to an infected patient is rising at an exponential pace. In Vacaville, California, alone, one case — the first documented instance of community transmission in the U.S. — left more than 200 hospital workers under quarantine and unable to work for weeks.
Across California, dozens more health care workers have been ordered home because of possible contagion in response to more than 80 confirmed cases as of Sunday afternoon. In Kirkland, Washington, more than a quarter of the city’s fire department was quarantined after exposure to a handful of infected patients at the Life Care Center nursing home.
With the number of confirmed COVID-19 cases mushrooming by the day, a quarantine response of this magnitude would quickly leave the health care system short-staffed and overwhelmed.
. . .
National Nurses United, a union representing more than 150,000 nurses, recently held a news conference to call on hospitals to better protect their workers. Of the 6,500 nurses who participated in a survey the union circulated, fewer than half said they had gotten instruction in how to recognize and respond to possible cases of COVID-19. Just 30% said their employer has sufficient protective equipment on hand to protect staff if there were a surge in infected patients.
Again, more at the link.
We need to spare more than just a thought for our health care and emergency response personnel. They’re on the front lines in the fight against this disease, and many of them are already paying the price through becoming infected. In Italy, many health care workers are no longer going home to their families, for fear of infecting them. Instead, they’re effectively living at work, quarantining themselves along with the sick. That’s dedication with a capital “D”. I hope that some sort of recognition will be given to them when that’s possible, preferably one involving high-denomination dollar bills. They’ll have earned it the hard way. We should be more than grateful to them.
We should be particularly thankful for those medics, nurses and doctors who are trying to keep us informed, and bring us accurate information. There are many of them, but one who stands out is Aesop, writing at his blog Raconteur Report. (His latest article is here, and is well worth reading.) Aesop, from this non-medic, a grateful doff o’ the hat, and prayers for your safety. Please keep us informed – and take care of yourself!
We can expect a doubling of cases every six days, according to several epidemiological studies. Confirmed cases may appear to rise faster (or slower) in the short term as diagnostic capabilities are ramped up (or not), but this is how fast we can expect actual new cases to rise in the absence of substantial mitigation measures.
That means we are looking at about 1 million U.S. cases by the end of April; 2 million by May 7; 4 million by May 13; and so on.
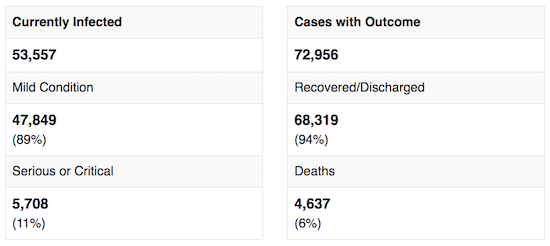
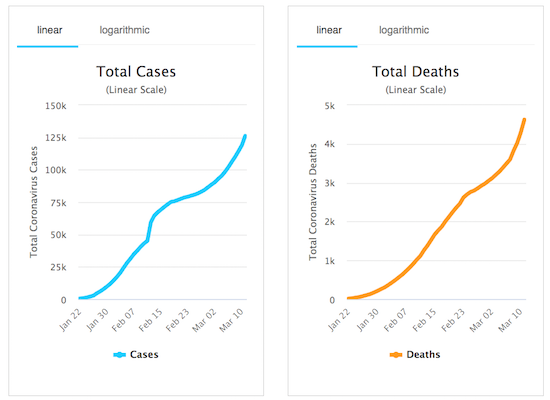
The latest figures from Worldometer, shown in graphical format below, offer no signs of any major reduction in the infection rate worldwide, even though some countries are reporting successes. (Of course, those figures are only as reliable as the countries reporting them, and we all know about how untrustworthy some of those numbers are. Bear in mind that errors are likely to be on the conservative, optimistic side of reality. Things may be worse than these figures convey.)
There are signs that the death rate from COVID-19 may be better than the raw numbers above indicate. South Korea, in particular, is showing an encouraging trend.
“If we can test more people – whether they have no symptoms, mild or severe disease – the results, including the case fatality rate, are more accurate and representative when the whole disease spectrum is taken into consideration,” said David Hui Shu-cheong, an expert in respiratory medicine at the Chinese University of Hong Kong.
“Most countries just focus on testing the hospitalized patients who obviously have more severe disease, and [thus] the fatality rate is high.”
South Korea, which introduced a system to grant the rapid approval of testing kits for viruses after 2015’s outbreak of Middle East respiratory syndrome in the country that killed 38 people, has won international plaudits for the scale and speed of its screening regime, which includes drive-through stations that can test members of the public in minutes.
. . .
One question puzzling disease experts has been Covid-19’s mortality rate, which has seemingly ranged from 2-3% in China up to 10% in Iran, based on official numbers . . . World Health Organization Director-General Tedros Adhanom Ghebreyesus on Tuesday said the global mortality rate from Covid-19 recorded so far was about 3.4%, higher than previous estimates.
Yet in South Korea … the mortality rate appears to be hovering around 0.64%.
While this is still several times more lethal than seasonal influenza, which kills about 0.1% of the people it infects – 30,000-40,000 people in the US alone each year – South Korea’s rate is far lower than that seen elsewhere.
Let’s hope that in countries with advanced health care systems, that pattern is repeated.
All right, that’s the health care side of things. What about the impact of COVID-19 on the economy? That’s not looking very good at all. Most of us will by now have heard or read about President Trump’s address to the nation last night. I think he’s doing the right thing by shutting down easy access to this nation from Europe, just as he did the right thing, early in this crisis, by closing our borders to traffic from China and other early-onset nations. His actions have probably protected us far more than we know, and we should be grateful for them. Ignore the Democratic Party and their mainstream media allies as they try to blame the entire crisis on him. They’re lying, as usual – but then we already knew that. We can expect nothing else from them. It’s the way they roll.
I’m sure that’s why the White House decided to classify all high-level discussions about the coronavirus. If you knew the media and your political opponents would scrutinize every word, looking for ammunition to shoot at you to discredit you and your policies, and help your political opponents, wouldn’t you have done the same? The media may try to classify this as “an unusual step that has restricted information and hampered the U.S. government’s response to the contagion”, but it’s not. It’s basic common sense. Those who need to know, do know. Those who don’t need to know can wait until an appropriate time to be told. Officials don’t have time to waste endlessly briefing the media when they should be – and are – working to contain the crisis.
Of course, a lot of the information out there about COVID-19 is suspect. That includes many alarmist articles in the mainstream media, but also reports in the “alternative” media, and allegedly “expert” articles, even books, by people we’ve never heard of before. A number of hastily-written books are offering “expert advice” that turns out to be nothing more than compilations of news articles. Shysters, fraudsters and imposters have always been with us, and they’ll try to take advantage of this crisis, just as they have every previous crisis. Caveat emptor, and be careful whom you trust to give you accurate information. (Yes, that includes me. That’s why I try to back up every claim I make with a source reference, so you can check it for yourself, and decide whether or not I’m giving you good information. I can make mistakes, too!)
The economic impact of COVID-19 is already massive, and is likely to get much, much worse. In fact, I think the biggest danger to the First World may well be the damage to our economies from this disease. Supply chains all over the world have been disrupted, and show no signs of recovery as yet.
Notably, nearly 75 percent of companies report supply chain disruptions in some capacity due to coronavirus-related transportation restrictions, and more than 80 percent believe that their organization will experience some impact because of COVID-19 disruptions. Of those, one in six (16%) companies report adjusting revenue targets downward an average of 5.6 percent due to the coronavirus.
“The story the data tells is that companies are faced with a lengthy recovery to normal operations in the wake of the virus outbreak,” said Thomas W. Derry, Chief Executive Officer of ISM. “For a majority of U.S. businesses, lead times have doubled, and that shortage is compounded by the shortage of air and ocean freight options to move product to the United States — even if they can get orders filled.”
Primary reported supply chain impacts include the following:
- 57 percent noted longer lead times for tier-1 China-sourced components, with average lead times more than doubling compared to the end of 2019.
- Manufacturers in China report operating at 50 percent capacity with 56 percent of normal staff.
- More than 44 percent of respondents do not have a plan in place to address supply disruption from China. Of those, a majority (23 percent of respondents) report current disruptions.
- Of the companies expecting supply chain impacts, the severity anticipated increases after the first quarter of 2020.
- Six in 10 (62%) respondents are experiencing delays in receiving orders from China.
- More than half (53%) are having difficulty getting supply chain information from China.
- Nearly one-half are experiencing delays moving goods within China (48%).
- Almost one-half (46%) report delays loading goods at Chinese ports.
Rail traffic figures in the USA bear this out.
- In February 2020, US railroad intermodal (i.e. container) shipments were down 8.9% from the same month in 2019.
- For the week ending March 7, intermodal (container) traffic was down 14.9% compared to the same period in 2019.
This has led to “panic buying” in many countries, including our own. I had to laugh at this editorial cartoon. Full marks to the artist!

EDITED TO ADD: Thanks to Cedar Sanderson, I learned that this cartoon is from Theo Moudakis, editorial cartoonist for the Toronto Star newspaper in Canada. I’m going to look for more of his work. If it’s all this good, he’ll become one of my daily reads.
The drop in container traffic is going to get worse. Most of those containers referenced above were shipped from China before, and during the early stages of, the coronavirus epidemic there. Very few have been shipped in the past month, and many sailings of container vessels have been canceled due to lack of traffic. That’s now beginning to show up at our harbors, as we discussed last week. Remember that containers are used to bring in most of our manufactured imports from overseas. GCaptain reports:
At the neighboring ports of Los Angeles and Long Beach, the two busiest in the U.S. and the main entry points for Chinese goods, work shifts so far this year have dropped 21% compared with the same period a year ago, according to the Pacific Maritime Association. Both facilities just released their February container volumes: Long Beach’s imports dropped 18% from a year earlier, L.A.’s sank 23%.
More broadly, U.S. seaports could see slowdowns of as much as 20% continue into March and much of April, according to the American Association of Port Authorities. The same trend is seen in more distant places, with Rotterdam — Europe’s economic gateway to Asia and beyond — seeing a similar cut of about 20%.
In another report, GCaptain notes:
While the global economy is reeling from the spreading virus, seaports are a bellwether for trade because they handle a hefty 90% of all world shipping. The squeeze on ports like Los Angeles, the biggest in the U.S. for container traffic, illustrates the vast potential for economic harm from a virus-induced slowdown.
. . .
“Alarm is the word,” said Jock O’Connell, a foreign trade consultant in California. “The demand for longshore labor has been down, but the real victims are the truck drivers who get paid by the load and the warehouse workers, who process goods.”
. . .
Los Angeles, especially, is coping with an overload of shipping containers lately and running out of places to store them. The outbreak has disrupted the usual balance of trips between the U.S. and Asia, with too few vessels arriving in L.A. to take the containers back to Asia.
Do please note that last report. Truck drivers and warehouse personnel are likely to be very hard hit by this downturn, as are retail staff. Also, if Chinese factories return to production, but don’t have enough containers to pack their goods for export, we’re still going to be hurting for them. It’s going to be tough for several months at least.
On the other hand, Tom Luongo notes a potentially positive side to the economic downturn.
… the choice between inflation and deflation is a non-choice. They are two sides of the same coin. The question is only who benefits from which side.
Those in power always choose inflation because, in their minds, it is less upsetting to the social order than deflation.
And their power rests on maintaining the current social order.
Deflation benefits savers and, frankly, normal people who don’t have access to new money at the lowest available prices, those set by the Fed’s discount window.
It gives them back power stolen from them through inflation.
. . .
I like to think of global trade in real goods as the M0, or base money, of the global financial system and the oil trade that which is the M0 of that.
All of the credit, government debt, corporate debt, stocks prices and the rest are simply credit derivatives in a fractional reserve banking system of that fundamental trade in goods and services.
And the value of the monetary base for global trade was just halved in the last six weeks with the price of oil crashing from $70 per barrel (Brent) to around $35.
. . .
This move will force trillions in debt to be liquidated. Prices will adjust down. Debtor economies which are in desperate need of U.S. dollars, just had their energy costs cut in half, making it far easier for real people to get to work, buy food, pay off debt and build a life for themselves.
Those who have saved in real assets, like gold, just saw their wealth double in real terms over the past few days.
. . .
The number of dollars you have is irrelevant. It is only what you can buy with that money that gives that money power.
Deflation is the transfer of wealth back from debtors to savers through the increase in purchasing power of your money and the liquidation of over-priced assets by desperate debtors trying to remain solvent.
Go read the whole thing. I think he makes a good point.
Peter
Peter, Longtime ER nurse here.
Regarding hospitals, ours is hopeless (north of Dayton Oh). I've been trying to nudge managers, and getting nowhere. Just a 'go-back-to-your-trench-and-stop-asking-questions.' The health department had a meeting yesterday with managers and EMS and basically told everyone, 'there is no plan, we're all gonna die.' Our EMS guys are ready to walk.
Yesterday, I asked about separating people with triage tents out front,so Covid patients don't end up contaminating the whole ER when they walk in, was told there's no need. "They'll be given a mask by the triage nurse." A surgical mask.
I asked about N95s, was told we only have 70 in the whole hospital, and nobody to fit-test anymore bc when we got swallowed up by 800lb gorilla hospital,it was deemed unnecessary. We have over twice that many staff in ER, let alone ICU, RT etc.
I asked about using PACU as ICU overflow as they have vents there; was told 'No, we're not doing that.'
I asked about drive-up testing, like they're doing in SKorea, Germany, England, was looked at like I had 3 heads and told it was silly. And, the "CDC only provided the state with 150 test kits." I said, "what about private labs, or the State?" She pressed her lips together and told me firmly, "We're using the CDC guidelines! Regular surgical masks will be sufficient. You can't get this if you're standing 4 feet away." Then she walked off.
I was left slackjawed. I've been researching the hell out of this, and, yes, you can. They've already done mapping studies of where people were sitting on busses and how the virus was spread to other passengers at the front of the bus A HALF HOUR AFTER the Covid guy at the back of the bus got off. (Surveillance state can be useful in epidemiology.) She refuses to look at the pictures of hospitals everywhere else, where they're in full hazmat gear. Oh, and our triage nurse isn't going to be wearing a mask because it 'throws people off.'
If I felt like we really had a voice, I'd probs be one of the ones living at the hospital and working around the clock. But this huge corporation just uses up nurses like kleenex – 'there's plenty more where that came from.' Our department has burned through 45 of them in the last YEAR. I don't even bother learning their names anymore. It's not about altruism, and saving people. I really don't feel like putting my health and life on the line for a company that isn't interested in protecting me and uses staff like disposable cogs. So, after I work my shift tomorrow, I'm taking daughter #2 and going on a two-week backpacking trip to south Texas. Wanna see the bluebonnets.
Jennifer
Re Healthcare workers: Czechoslovakia is considering using senior medical students to fill in for healthcare workers who are sick or need to stay home to provide child care. There's also talk of using students in elementary education to assist in pediatrics and child care.
Johns Hopkins GIS COVID-19 tracker: https://gisanddata.maps.arcgis.com/apps/opsdashboard/index.html#/bda7594740fd40299423467b48e9ecf6
Arguably Wrong's simple epidemiological model, with code: https://arguablywrong.home.blog/2020/03/10/epidemiological-modeling/
Has no one noticed that South Korea has drive-through tests with immediate results while America needed CDC permission to develop and bring to market a test which takes only "8 to 14 days" to provide results?
Are we Americans actually so inefficient, or is it the "dumbing down" caused by nanny-state over-regulation which is accelerating our slide into 3rd-world status?
The second, sadly.
On my way back from Blighty.
They’re pissed in Europe right now as the news of the travel ban breaks.
UK BBC Today program (Thurs am) French govt minister responding to Trumps travel ban. Effectively said US public must do something to curb this “mad president” . BBC interviewer said perhaps the us govt should use 25th amendment to depose Trump. I didn’t hear the same approbation about Italy essentially closing its borders.
The establishment in Europe dislikes Trump more than the Dems in US if that were possible. The frog said he would simply get on the Eurostar and travel to London to then fly to New York. His point was that because the ban wouldn’t be 100% effective then it shouldn’t be enacted at all…
I understand that this situation is making shipping and economic impacts, however a simple comparison of year to year shipping at Long Beach and LA isn't appropriate here – since the Panama Canal expansion opened several years ago, expensive West Coast ports have been losing significant amounts of business to cheaper Gulf and East coast ports that are closer to more customers. The last numbers I read were a downturn of about 7% a year on the West Coast due to this trend.
Peter (& co.),
1) You're welcome. I do what I do.
2) Medical triage: I warned people what the likeliest answer is going to be a couple of days ago:
https://raconteurreport.blogspot.com/2020/03/kung-flu-victims-bus-undercarriage.html
Swallow hard. If I thought there was a better answer, I'd suggest it, but I can't see any way around it.
As far as ICU beds, I concur that when push comes to shove, (and within a week, or a month, it will) we'll do the exact same thing. Younger patients will get first priority, and the over-60 crowd will get last priority.
There simply aren't that many isolation beds in most hospitals to start with, and we're not going to expend those resources on 80 year olds when there are 50 year olds (or, God forbid, younger patients) in the same boat.
3) I'll be blogging regularly. Status updates as appropriate.
This is in everyone's community now.
Minimize interactions, or self-quarantine, as necessary and possible.
Wash your hands.
Don't touch your face.
Get your rest.
Take your vitamins.
See you on the other side, I hope.
Best wishes to one and all.
You said the media and his (Trump) political enemies, the media IS part of his political enemies…
Maybe it will help to spread this meme:
Fight TV-PANIC virus
JWM
Two things that may mitigate all the freakout.
1. ComChinese workers are heading back to work. End of March should see about 50-75% of the workers back on full time, with end of April being 100%. It not affecting younger people as easily is making this possible. Though they may have lost some of those older workers who know everything (you know, the ones US companies RIF in order to 'save' money and then realize (maybe) that those workers were what kept the system running
2. Italy and other places that have seen a lot of death have lots and lots of old people living in cramped quarters (a nice apartment in Europe is a small and cramped apartment in the US of A.) The combination of old people with respiratory issues (like in ComChina and Italy and in US city warrens) and closer contact make these places great places for Corona-chan.
Yes, we don't need to import any more diseased people from Europe or Asia or Africa.
Yes, we need to light a fire under the CDC to get same-day test kits and proper equipment.
Yes, we will see some economic issues from this. We saw economic issues from the Ebola outbreaks that never really hit our shores.
Worry and plan and expect the worst. That's how you attack a 'pandemic,' whether really dangerous, somewhat dangerous or not really dangerous.
Soon to be FUBARE (FUBAR Everywhere)…
Peter, that comic was done by Theo Moudakis. https://twitter.com/TheoMoudakis/status/1237709867005214725
Just walked into one of the major hospitals here in Phoenix AZ to get some medical records.. Nobody is wearing masks. Not the doctors or nurses, not the cafeteria workers, not even the guys emptying the trash cans. Also, I saw only two people wearing gloves, a cashier and a sanitation worker.
The normalcy bias is STRONG here. Even after the travel restrictions, the event cancellations, the school closings, the NBA cancelling the rest of their season, and the WHO declaring this to be a worldwide pandemic, most people here, including healthcare professionals, are NOT taking this seriously.
I believe the biggest problem we face is the inability of people, including the CDC and other .gov agencies, to wrap their minds around what is actually happening. After all, there has not been a worldwide pandemic in 100 years. Nobody is still alive who remembers what it was like. And nobody who is alive today can imagine it. Normalcy bias is going to kill many millions.
@Cedar: Thanks! I'll update the article to credit him.
On the mask issue / use in the us – I’m not sure they are even available in the us. The majority of masks seemed to have been made in China.
How much of the 'down 20%' shipping-wise is continued slow-down from the change in the trade situation? Wasn't this the time last year all the businesses were ordering extra because import fees & tariffs were going up?
@George,
It's administration.
They've got their heads clenched so high and tight on this it's going to take walk-outs, or threats of same, before they break suction.
It isn't helping that at least 75% of medical staff (doctors) are spewing the same "it's just the flu" happygas bilge, because they aren't experiencing Italy's collapse of healthcare right in their faces. Yet.
Survivors will study the stupidity rampant for decades, but in the meantime, this afflicts older folks more severely.
And the median age of RNs in this country is 50.
If you think it's bad now, wait until 10-75% of the nursing staff is out either sick, or self-quarantining.
We've done health care without nurses. It was called the Crimean War.
And it only killed 60% of everyone outright, from preventable causes like dysentery and cholera.
This is going to be fun. Not.
As said above, it's been 100 years. No one has experience or sensitivity. Also, because we have been hearing it affects the elderly like any other flu, many people think it won't affect them.
I'm in Georgia and the Governor gave a speech yesterday, protect the elderly. What he didn't say is protect those who help the elderly. Nor did he talk about what happens when hospitals are overwhelmed. He did say we can only do 50 tests a day, but should be up to 100 by end of next week. What the Firetruck? Atlanta is home of the CDC and we are that limited in ability to test.
What is bad about this virus is how long people are asymptomatic and spreading the disease. Still a lot of conflicting information and with low test capability this thing is going to spread. Add in normalcy bias and things will get worse. By my math we are doubling every 4 days, but I think this is impacted by a limited ability to test.
On the positive side traffic is down and even if the toilet paper is gone, there is still plenty of food on the shelf. Prepare for more than 30 days, you will be glad you did if thing gets out of hand.
I'm hoping that Trump will escalate sooner rather than later, but politics is the art of the possible and he has his hands full politically.
Until there is a vaccine we can't change how many people will get the virus, we can only change the timing. We can't afford to have all our utility workers go out sick and have the lights go off (another industry where there is a high median age). If we swamp our hospitals, then we will have to pull an Italy and deny treatment to a lot of people.
As the greatest country on earth we need to meet the challenges of:
Masks for everyone (make them out of old shirts, poor is much better than nothing)
Rapid manufacture of equipment needed to support breathing (relax regulations as needed, saving 8/10 is better than 0/10 with no equipment)
Quickly training some assistants for limited health services
Getting drug production started back up (See how well globalism worked when other countries decide they need to take care of their own people first)